What is Model of Human Occupation (MOHO) by Gary Kielhofner
- Developed by Kielhofner, the Model of Human Occupation (MOHO) is an occupation-based model that explains how people engage in occupation in daily life.
- MOHO is grounded in systems theory (open systems), viewing humans holistically within physical, mental, and social environments.
- The model of human occupation (or MOHO) suggests that occupational behavior arises from the interaction of volition, habituation, and performance capacity.
- Occupational therapy practitioners (OTs) and certified occupational therapy assistants draw on MOHO theory to guide assessment, intervention, and evaluation.
- Kielhofner’s Model of Human Occupation is widely used in occupational therapy practice across settings such as rehabilitation programs, community based organizations, work programs, and programs for persons with traumatic brain injury, persons living with AIDS, adults who are homeless, and children with attention deficit hyperactivity disorder (ADHD).
- As a definitive resource on the theory, MOHO also emphasizes meaningful activities, the role of environment, and client-centered occupation focus.
Key Concepts of the MOHO
- Three interrelated components (central to MOHO / Model of Human Occupation):
• Volition — the drive to choose and engage in occupation, including personal causation, values, and interests.
• Habituation — the routines, roles, and patterns (“routine / pattern”) through which occupation is organized.
• Performance capacity (or capacity) — the physical and mental abilities that underlie skilled occupational performance. - Volition (in depth)
• Personal causation: beliefs about one’s capabilities and effectiveness in doing occupations.
• Interests: what the person finds enjoyable or satisfying.
• Values: what is meaningful, guiding choice of occupations.
• In MOHO, volition explains how occupations are motivated—the model of human occupation frames the motivational system. - Habituation (in depth)
• Roles: social or personally meaningful identities (e.g., student, worker, parent).
• Routines / patterns: predictable sequences of actions (daily structure).
• The habituation subsystem shapes how occupation is organized over time. - Performance Capacity (in depth)
• Refers to physical and mental abilities that underlie skilled occupational behavior (e.g., strength, cognition, motor control).
• Performance capacity refers to the functional body systems supporting occupational performance.
• In MOHO, health or disease may impair these abilities and thus affect occupational behavior. - Open systems & holistic perspective
• MOHO treats human beings as open systems, constantly interacting with physical and social environments.
• The model of human occupation encourages holistic thinking: not just task or impairment but person + environment + occupation.
• The theory and application of MOHO reflect occupation-focused, client-centered, evidence-based approaches. - Model aims and overarching logic
• MOHO aims to predict, explain, and influence occupational behavior.
• It offers practical tools, a structure for assessment and intervention.
• Kielhofner’s MOHO (including the 6th edition) continues to refine concepts and applications in occupational therapy across populations. - Relevance to occupational therapy practitioners
• Occupational therapists use the Model of Human Occupation as a frame of reference in practice.
• Because MOHO is qualitative and quantitative, it supports practical tools and evidence-based work in OT settings.
• It supports occupational therapy services across rehabilitation, community, and clinical settings.
Dissertation Services
Expert support at every stage.
- Topic and proposal help
- Step-by-step writing support
- Editing, formatting, proofreading
Free Consultation
Talk to our dissertation experts.
- One-on-one discussion
- Advice on structure and citations
- Guidance tailored to your program
Occupational Adaptation in the Context of MOHO
- Definition of Occupational Adaptation
• Occupational adaptation refers to how individuals adjust or respond to internal or external challenges in pursuing occupation.
• In MOHO, adaptation is a dynamic process interwoven with volition, habituation, and performance capacity. - How MOHO incorporates adaptation
• The model of human occupation sees adaptation as a continuous, iterative response to changes in capabilities, environment, or roles.
• MOHO recognizes that when performance capacity is reduced (e.g., in traumatic brain injury or chronic disease), occupational adaptation is essential.
• Occupational therapy practice guided by MOHO supports clients to adapt their habits, roles, patterns, or environment to maintain occupational performance. - Mechanisms of adaptation in MOHO
• Altering routines / patterns (habituation) to accommodate new limitations or opportunities.
• Modifying how occupations are done (using compensatory strategies).
• Reevaluating volitional choices: sometimes shifting interests or values in light of new constraints.
• Gradual reorganization of roles: adopting new or modified roles compatible with current capacity. - Examples in practice populations
• In clients with attention deficit hyperactivity disorder, occupational adaptation might involve restructuring routines, introducing external scaffolding, or adjusting task demands.
• In persons with traumatic brain injury, adaptation may include redesigning work programs, compensatory methods, or environmental supports.
• For adults with chronic conditions (e.g. chronic pain, neurological disease), MOHO‐based occupational adaptation focuses on sustaining meaningful occupation by modifying tasks or environment. - Role of occupational therapists / occupational therapy practitioners
• Occupational therapists help clients reflect on performance challenges, volitional shifts, and role changes.
• Using MOHO theory and application, OTs guide clients in emerging adaptation strategies.
• OTs integrate occupational adaptation within occupational therapy practice to enable continued participation. - Evidence and theory supporting adaptation in MOHO
• MOHO as an evidence-based model includes research showing adaptation processes in diverse populations.
• The 6th edition of MOHO highlights updated theory and application of occupational adaptation.
• As a definitive resource on the theory, MOHO’s conceptualization of adaptation gives a robust frame of reference for clinical decision-making. - Benefits of adaptation approach
• Helps clients maintain occupational identity even in face of limitations.
• Encourages resilience, flexibility, and long-term engagement in meaningful activities.
• Facilitates sustainable occupational performance over the life span, even with changing capacity. - Limits and considerations
• Adaptation must balance between challenge and overload—therapist must calibrate interventions carefully.
• External constraints (e.g., environment, resources) may limit adaptation options.
• Not all occupational issues resolve via adaptation—sometimes remediation or compensation is needed.
Integrating MOHO into Occupational Therapy Practice
- Why adopt MOHO in practice
• The Model of Human Occupation (MOHO) offers a robust, client-centered frame of reference for occupational therapy services.
• Occupational therapy practitioners (OTs/OTAs) find MOHO useful because it blends theory and application, guiding both assessment and intervention.
• Kielhofner’s model of human occupation is widely taught in entry-level occupational therapy curricula (including the analysis of entry-level occupational) and in certification preparation. - Steps to integrate MOHO
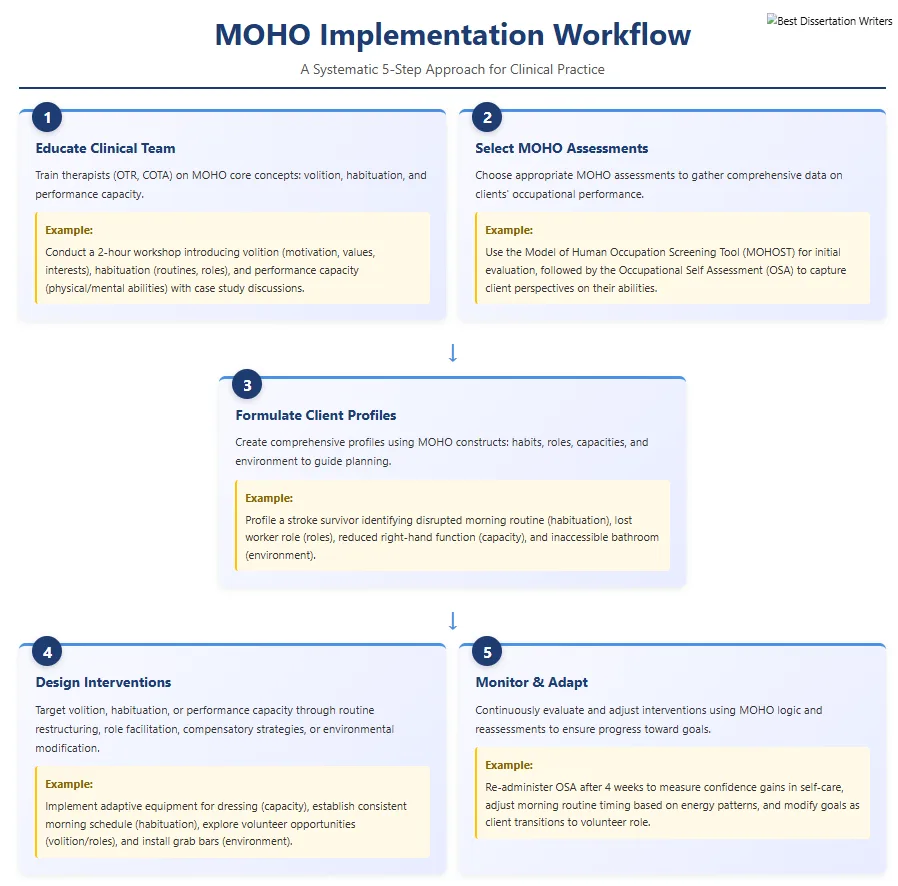
- Educate the clinical team (therapists registered and certified, therapist registered and certified occupational, certified occupational therapy assistants) about MOHO core concepts (volition, habituation, performance capacity).
- Select appropriate MOHO assessments (see next section) to gather data on clients’ occupational performance.
- Formulate client profiles using MOHO constructs (habits, roles, capacities, environment) to guide intervention planning.
- Design interventions that target volition, habituation, or performance capacity—for example, restructuring routines, facilitating new roles, compensatory strategies, strength/cognitive rehabilitation, environmental modification.
- Monitor, evaluate, and adapt interventions over time using MOHO logic and reassessments.
- Application in different settings
• In rehabilitation programs, OTs use MOHO to support clients recovering from injury or illness (e.g. TBI).
• In community based organizations or work programs, MOHO helps design occupation-based interventions for adults who are homeless or living with AIDS.
• In mental health or pediatric practice (e.g. children with ADHD), MOHO offers a framework for adjusting routines, roles, and volitional supports. - Bridging theory and practice
• MOHO is not purely theoretical—it provides practical tools and a logic to guide real interventions.
• The definitive resource on the theory, including the 6th edition, gives updated evidence and case examples for occupational therapy practice.
• Occupational therapists balance occupation-based model thinking with hands-on strategies for capacity improvement and environmental adaptation. - Supporting professional credentials
• Knowing MOHO strengthens one’s foundation for the National Board for Certification in Occupational Therapy and Board for Certification in Occupational Therapy exams.
• Mastery of MOHO theory helps entry-level occupational therapist registered candidates in certification preparation.
• It also supports continuing education and advanced practice as a practice model central to OT identity. - Challenges and considerations
• Some settings with strong biomedical orientation may undervalue holistic occupation models.
• Implementation takes time—therapists may need training, supervision, and adaptation of documentation systems.
• Cultural or contextual factors may require modification of MOHO constructs or language for diverse clients.
• OTs should integrate MOHO flexibly—combining with other approaches (e.g. biomechanical, cognitive behavioral) when needed. - Outlook and future directions
• Ongoing updates (e.g. future editions following 6th edition) will refine MOHO.
• More empirical research will continue to strengthen the evidence base.
• As OT continues to evolve, MOHO remains a central occupation-focused, client-centered guide for practice.
Example of Integrating MOHO into Occupational Therapy Practice
Integrating the Model of Human Occupation (MOHO) into occupational therapy practice allows practitioners to view clients through a holistic, client-centered, and evidence-based lens. Developed by Gary Kielhofner, MOHO emphasizes that occupation is the primary means through which humans achieve health and well-being. It provides a frame of reference that guides therapists in assessment, intervention, and evaluation by examining the dynamic interaction of volition, habituation, performance capacity, and the environment.
1. Understanding the Core Concepts
Volition refers to the client’s motivation for engaging in meaningful activities. Therapists using MOHO explore a client’s personal causation (beliefs about ability), values (what matters most), and interests (what the client enjoys). Habituation represents the routines, habits, and roles that structure everyday life. MOHO encourages therapists to analyze how these patterns help or hinder occupational performance. Performance capacity refers to the physical and mental abilities that underlie skilled occupational behavior. Finally, the environment—both physical and social—shapes and supports occupational participation.
By understanding these subsystems, occupational therapists (OTs) can develop a clear picture of how a person’s internal motivation interacts with external demands. This open-systems perspective reflects the holistic philosophy that distinguishes MOHO from reductionist biomedical models.
2. Applying MOHO in Assessment
In practical terms, occupational therapy practitioners use MOHO assessments to evaluate clients systematically. Instruments such as the Model of Human Occupation Screening Tool (MOHOST), Occupational Self-Assessment (OSA), and Occupational Performance History Interview (OPHI-II) gather data about volition, roles, and performance capacity. For example, when working with a client recovering from a traumatic brain injury, the OT may use the OSA to understand which occupations the client values and how they perceive their current abilities. These tools provide both qualitative and quantitative data, helping therapists identify areas of strength and barriers to participation.
3. Designing Client-Centered Interventions
Once assessment results are analyzed, therapists design occupation-based interventions aligned with the client’s volitional and habitual patterns. For instance, in adults with chronic illness, the OT might focus on restructuring daily routines (habituation) and introducing meaningful activities that support self-efficacy (volition). In children with attention deficit hyperactivity disorder, the intervention might target consistent routines, environmental adjustments, and strategies to enhance sustained engagement.
Because MOHO also emphasizes occupational adaptation, interventions are adjusted as clients’ abilities and circumstances evolve. The therapist acts as a collaborator—guiding, motivating, and modifying the therapeutic process based on feedback and progress.
4. Bridging Theory and Application
The theory and application of Kielhofner’s Model of Human Occupation translate directly into practice by providing a framework for reasoning. Therapists can ask: What motivates this client? How do routines shape behavior? What physical and mental abilities influence performance? These reflective questions enable evidence-based, client-centered decision-making.
In rehabilitation programs and community-based organizations, MOHO helps structure interventions for persons living with AIDS, adults who are homeless, or persons with traumatic brain injury. The model guides therapists to build competence gradually, address volitional barriers, and foster occupational identity—the sense of who one is through occupation.
5. Professional Growth and Certification
Understanding and using MOHO benefits both clients and practitioners. Students preparing for the National Board for Certification in Occupational Therapy (NBCOT) or the Board for Certification in Occupational Therapy gain a stronger conceptual base for exams and practice. MOHO aligns with competencies expected of entry-level occupational therapist registered and certified professionals, reinforcing evidence-based reasoning and holistic care.
6. The Value of MOHO in Modern Practice
The 6th edition of the Model of Human Occupation expands its applicability with new case studies, research evidence, and practical tools. It remains the definitive resource on the theory for understanding how occupations are motivated, patterned, and performed. By consistently applying MOHO, therapists integrate theoretical knowledge with real-world problem solving—ensuring that each client’s rehabilitation is not just functional, but meaningful.
MOHO Assessments: Tools for Evaluating Occupational Performance
- Purpose and rationale
• MOHO assessments are instruments designed to operationalize the Model of Human Occupation in clinical and research settings.
• They translate MOHO theory and application into measurable data on occupation, habituation, volition, and performance capacity.
• They provide practical tools for occupational therapy practitioners to track changes, plan intervention, and evaluate outcomes. - Common MOHO assessments
• The Assessment of Communication and Interaction Skills (ACIS) – evaluates how clients communicate and interact in occupation.
• Occupational Self Assessment (OSA) – client self-report on perception of occupational competence and satisfaction.
• MOHOST (Model of Human Occupation Screening Tool) – a screening tool to identify strengths and barriers across MOHO subsystems.
• Volitional Questionnaire (VQ) – observational tool assessing volitional behavior and motivation.
• Occupational Performance History Interview (OPHI II / OPHI-VI, including 6th edition updates) – a semi-structured interview about a person’s occupational history, roles, routines.
• Role Checklist – helps clients list and reflect on current and past roles within MOHO framework. - Structure and domains
• These assessments typically cover volition, habituation, performance capacity, environment, occupational identity, and occupational competence.
• For example, OPHI II / OPHI-VI elicits narrative data about the client’s occupational identity, roles, habits, and life story.
• OSA captures how clients perceive their own skill and satisfaction in meaningful occupations—linking to occupational behavior. - Scoring, interpretation, and application
• Many MOHO assessments yield both qualitative and quantitative data—qualitative narratives plus scoring scales.
• Scores help clinicians prioritize intervention targets (e.g. volition, habituation, performance capacity).
• In occupational therapy practice, MOHO assessments inform intervention planning, goal setting, and evaluation over time. - Use across populations
• In children with attention deficit hyperactivity disorder, assessments may highlight difficulty sustaining routine or volitional engagement.
• In persons with traumatic brain injury, MOHO assessments reveal challenges in routines, role transitions, and performance capacity deficits.
• In adults with chronic illness, assessments detect erosion in occupational identity, habit, or volition, guiding adaptive intervention.
• In community based organizations, MOHO assessments help design occupation-based services for marginalized populations (e.g. persons living with AIDS, adults who are homeless). - Advantages of MOHO assessments
• Align directly with theory and application thus ensuring consistency.
• Client-centered: many instruments allow client voice (e.g., OSA, interview tools).
• Provide evidence-based structure to measure outcomes.
• Facilitate communication within interdisciplinary teams by framing occupational factors in MOHO terms. - Considerations and limitations
• Some MOHO assessments are time-intensive (e.g. OPHI interviews).
• Training is required to administer, interpret, and use reliably.
• Cultural and contextual factors may require adaptation of language or items.
• Not all settings support full MOHO assessment battery—therapists may need to select a subset for feasibility. - Role in certification and scholarly work
• Familiarity and skill in administering MOHO assessments support exam preparation for National Board for Certification in Occupational Therapy / Board for Certification in Occupational Therapy.
• In research, MOHO assessments contribute to the evidence base for MOHO theory and occupancy interventions.
• Use of MOHO assessments reinforces MOHO as a practice model in OT settings.
MOHO as a Frame of Reference in Modern Occupational Therapy
- What it means to be a frame of reference
• A frame of reference gives therapists a conceptual structure to guide assessment, intervention, and reasoning.
• Kielhofner’s MOHO functions as a robust frame of reference in occupational therapy practice. - Why MOHO is suited as a frame of reference
• It is theory-driven yet occupation-focused and client-centered.
• MOHO links theory and application, offering practical tools and guiding decision pathways.
• Because MOHO addresses volition, habituation, and performance capacity, it supports a holistic approach to occupational therapy interventions. - Role in guiding occupational therapy practice
• Occupational therapists use MOHO as the conceptual lens through which they see the client’s occupational profile (habits, roles, capacities, environment).
• Interventions are framed to influence one or more MOHO subsystems (volition, habituation, performance capacity).
• MOHO as a frame of reference helps therapists structure documentation, goal writing, and outcome evaluation in consistent ways.
- Advantages compared to other frames of reference
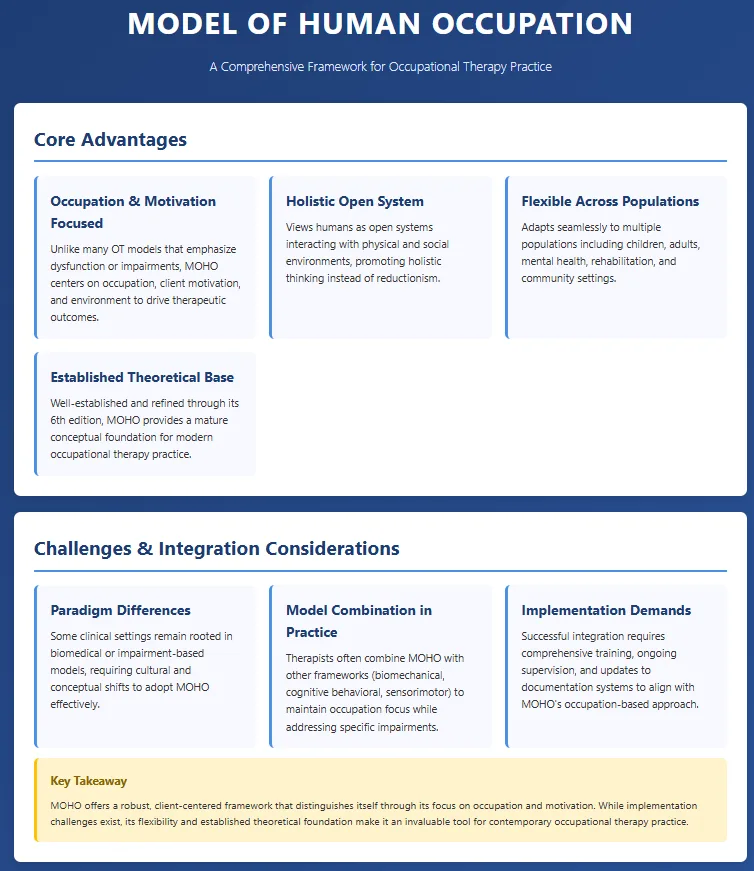
• Many OT models focus on dysfunction, impairments, or specific body systems. MOHO instead centers occupation, the client’s motivations, and environment.
• MOHO integrates the human as an open system, promoting holistic thinking rather than reductionistic views.
• It is flexible enough to be adapted across populations (children, adults, mental health, rehab, community).
• Because MOHO is well established (including its 6th edition), it provides a mature conceptual foundation for modern OT. - Challenges and integration with other models
• Some clinical settings are rooted in biomedical or impairment-based models; integrating MOHO may require paradigm shifts.
• Therapists may combine MOHO with other models (e.g. biomechanical, cognitive behavioral, sensorimotor) to address specific impairments while preserving occupation focus.
• Effective integration requires training, supervision, and change in documentation systems. - MOHO’s influence on occupational therapy education and certification
• MOHO is commonly taught in entry-level OT curricula (analysis of entry-level occupational therapist registered, certified).
• Understanding MOHO supports successful performance on the National Board for Certification in Occupational Therapy and Board for Certification in Occupational Therapy exams.
• It anchors many OT programs’ practice model frameworks, promoting consistency across cohorts and advancing the profession’s theoretical rigor. - Contemporary relevance and future directions
• As OT emphasizes occupational performance, client-centered care, and evidence-based practice, MOHO remains highly relevant.
• Ongoing research, case studies, and refinements (post-6th edition) continue to strengthen MOHO’s validity.
• Future iterations may expand integration with technology, cultural adaptation, and cross-disciplinary frameworks.
• For occupational therapy practitioners, MOHO’s enduring value is its capacity to unify theory, assessment, and intervention in an occupation-based, holistic system.
FAQs About MOHO in Occupational Therapy
-
What is the MOHO Model of Human Occupation?
The Model of Human Occupation (MOHO), developed by Gary Kielhofner, is a leading occupation-based model in occupational therapy. It explains how motivation (volition), habits and roles (habituation), abilities (performance capacity), and the environment interact to influence occupational performance. MOHO provides a holistic, client-centered, and evidence-based framework that guides therapists in promoting meaningful participation in everyday occupations.
-
What is the Model of Human Occupation Techniques?
MOHO techniques involve using standardized MOHO assessments, client interviews, and observation-based tools such as the MOHOST, OSA, and OPHI-II. Therapists apply these techniques to analyze volition, roles, and performance capacity, then design occupation-focused interventions that build motivation, structure habits, and enhance function. These evidence-based techniques ensure that occupational therapy practice remains client-centered, measurable, and grounded in Kielhofner’s MOHO theory.
-
What is the Model of Human Occupation and Mental Health?
The Model of Human Occupation (MOHO) plays a vital role in mental health occupational therapy. It helps therapists understand how clients’ motivation, routines, and abilities are affected by mental illness. MOHO interventions rebuild occupational identity, improve daily structure, and support adaptation in people with depression, anxiety, or schizophrenia. By focusing on meaningful activities, MOHO enhances recovery, self-efficacy, and overall psychosocial well-being.
-
What are the Four Elements of the MOHO?
The four elements of the Model of Human Occupation (MOHO) are volition, habituation, performance capacity, and the environment.
1. Volition drives motivation for occupation.
2. Habituation organizes daily habits and roles.
3. Performance capacity reflects physical and mental abilities for skilled occupational behavior.
4. The environment (physical and social) influences performance.
Together, these components make MOHO a holistic and occupation-centered model in occupational therapy practice.